

An old design of hinged knee replacement. Unfortunately this did not allow rotation of the knee, so early loosening was ultimately a problem.
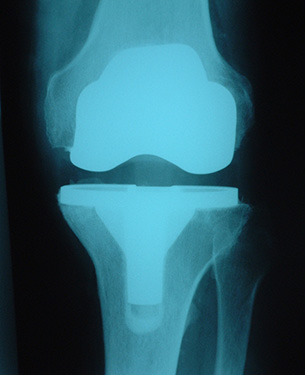
A more modern design of unconstrained total knee replacement which will allow some rotation between the femur and the tibia

An earlier design of partial (or unicompartmental) knee replacement. Here, only the osteoarthritic part of the knee is replaced and the rest is left alone.
In pre-replacement days the treatment of choice for severe arthritis of the knee was an arthrodesis (fusion). However, this was associated with other problems, such as extra strain being thrust on the back, hip and ankle, so surgeons looked for an alternative. Hemiarthroplasty was considered in the 1930s. This involved the replacement of half the joint, hence the term. Components were produced that replaced either the lower femur (thigh bone) or the upper tibia (shin bone). Unfortunately they had a high failure rate.
The next step was the creation of a design that replaced both femur and tibia. Initially both parts were linked with a hinge, on the assumption that the knee joint was indeed a hinge. However, although it is hinge-like, a significant degree of rotation also takes place at the knee as it bends and straightens. The hinged knee replacements thus began to loosen as they did not allow rotation to occur. Hinged replacements are still occasionally used to this day, though largely as revision components when all other avenues have been exhausted. If an artificial knee is hinged it is described as being constrained.
Because of the problems of constrained components, new designs were introduced that were semi-constrained. For such knees to be effective the major knee ligaments (cruciates and collaterals), or at least most of them, had to be intact. Stability after knee replacement was provided by the patient's own ligaments, rather than the replacement itself. In the early 1970s a design known as a total condylar implant was introduced. The shape of the tibial component looked to mimic the stabilising influence of the ligaments, although there was no hinge connection between femur and tibia. It was the success of the total condylar knee that paved the way for modern knee replacement surgery. The majority of designs today are of this type, albeit with minor modifications since the concept was first introduced.
Knee replacement components can be fixed to bone either with or without cement. The cement used is normally a material called polymethylmethacrylate (PMMA) and is identical to that used at cemented hip replacement. It may also contain impregnated antibiotic in order to minimise the chances of infection creeping in at surgery. Cementless components are normally coated with small beads, or irregularities, sometimes special chemicals, to encourage the patient's bone to grow into the component, thereby securing the artificial knee. Commonly the metal used for the femoral and tibial components is cobalt-chrome with a high-density polyethylene (HDPE) spacer used between the two to allow a low-friction articulation.
So much for total knee replacement. There is also a trend in some centres to only replace part of the knee, the area that is worst affected by arthritis. This is unicompartmental replacement. The attraction of this technique is that it allows the surgeon to conserve as much of the patient's bone as possible, thereby leaving room for further surgery in the years to come, should it ever be required. One form of unicompartmental replacement is the patellofemoral joint replacement. Sometimes arthritis can only affect the front of the knee, the patellofemoral joint. This, too, can be replaced in isolation, thereby leaving room for further revision surgery if required.
Why Replace The Knee?
There is only one major reason - pain. Other factors obviously influence a surgeon's decision. Such things as age, occupation, activity levels, weight, and previous knee disease all play a part.
The Princess Grace Hospital, 30 Devonshire Street, London, W1G 6PU | Enquiries: +44 (0)207 908 3777 | Fax: +44 (0)203 752 6501
enquiries@villarbajwa.com
© Villar Bajwa Practice (2015) | Terms & Conditions